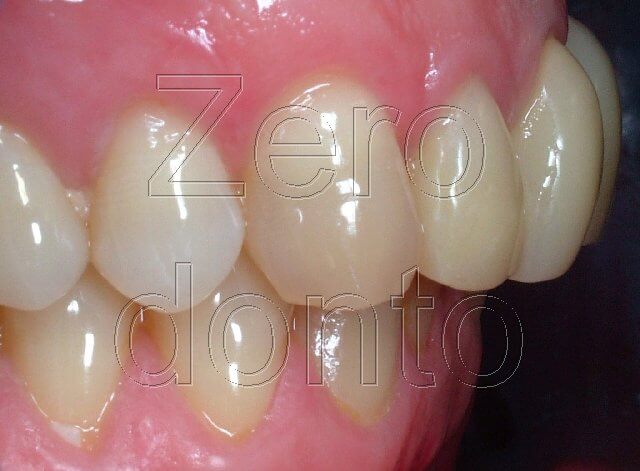
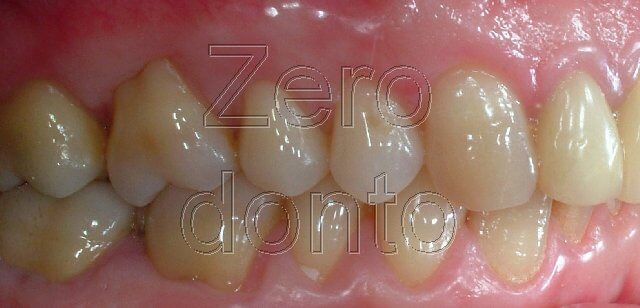
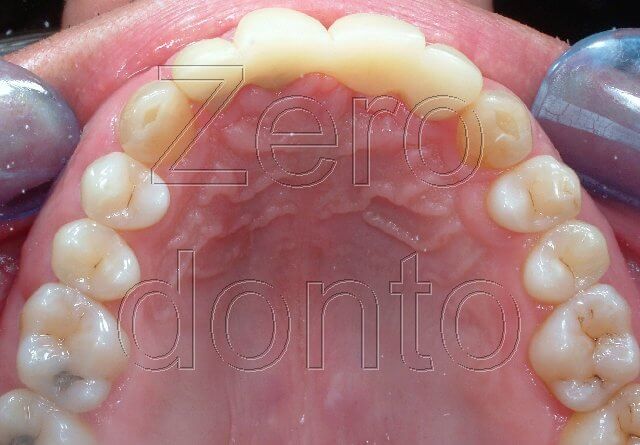
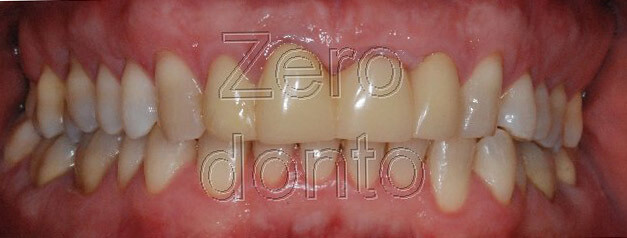
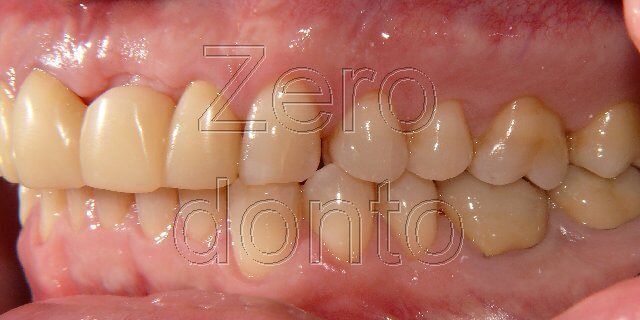
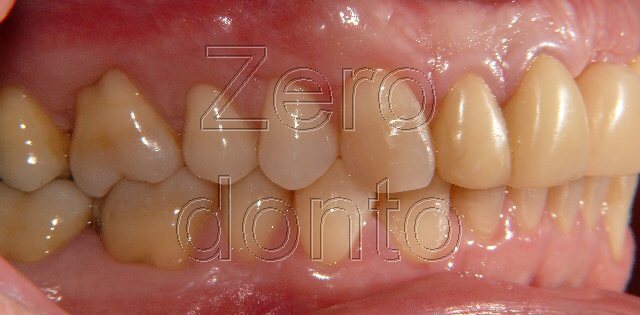
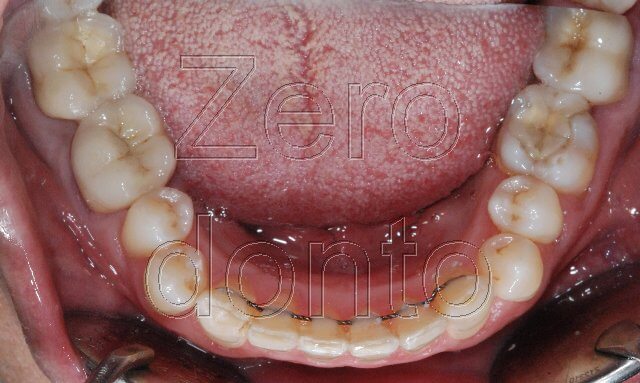
On examination, the patient revealed the following clinical evaluation (fig.1-7):
- Class I both molar right and left, Class I canine in the left side and canine to canine in the right side.
- Provisional bridge that involves the elements 12, 11 and 22 because of loss of the element 21 due to trauma
- Crowding in the lower arch
- OVB of 5mm, OVJ of 2 mm
- Periodontal health with absence of tooth pockets
- Different type of abrasion of the inferior canines. On the right much grater abrasion than left.




The patient demanded the alignment of the inferior dental arch to achieve with an invisible treatment and without feeling any pain or discomfort.
TREATMENT
The treatment has been made with the help of pre-activated retainers, a lingual tecnique without brackets conceived by Prof. Aldo Macchi and doctor Nunzio Cirulli (1-2) and subsequently performed by other authors (3-4). The pre-activated retainers has been used in order to expand the inter-canine area and to achieve the alignment of the lower front teeth. Thanks to the bridge made with a superior resin and previously unloaded, it has been possible to find space to bring the tooth elements into proper alignment through vestibular extension and without stripping.
During the first appointments some orthodontic records have been made, such as impressions for plaster models of the teeth, photographs and the radiographic exams have been prescribed. At the end, the orthodontic device has been applied.
Modelling active retainers
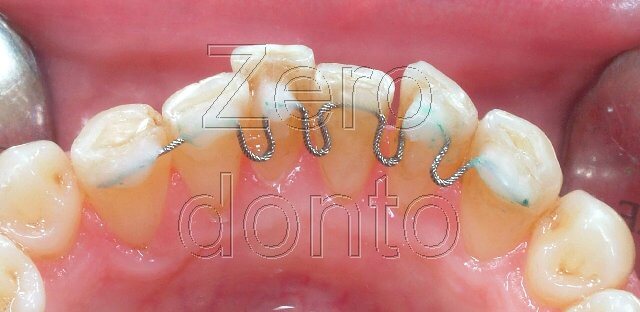
A 0.0175 inch twisted wire with round section made up of five threads was modelled to passively fit to the lingual aspect of lower teeth from canine to canine (fig. 8).
U-shaped handles with height of 3mms have been mesially and distally modelled to the teeth 41, 31, 32 and mesially modelled to the tooth 33.
These handles increase the elasticity of the wire allowing the expansion of the arch to make small vertical levelling.
Retainer activation
The thread has been activated inclining lingually the segment to be bonded to the teeth 41 and 32 and inclining vestibularly the segment to be bonded to the tooth 31.
Each U-shaped handle has been opened at about 1.5 mm.
Attachment Retainer
The lingual surfaces of the lower front teeth carefully cleaned have been etched for 30 seconds. The bondig agent has been applied each teeth and then polymerized for 20 seconds.
With the use of an utility probe the wire has been displaced to the tooth 31 maintaining the horizontal plan and then covered by a composite fluid of 1mm (Filtek Flow, 3M ESPEs). After we proceeded to polymerize for 20 sec.
Each of the mesial and distal handles have been closed at 1.5 mms to the element 41.
The thread has been bonded to the teeth 42 and 43 and covered by a composite of 1 mm. Note that during the procedure to close the handles it is important t to not overturn the thread that means not to displace it coronally or apically . The thread must maintain the horizontal plan all the time, otherwise it may occur to produce unwanted extrusive and intrusive forces!
Subsequently, the mesial and distal handles have been closed at almost 1.5 mm to the element 42 and the thread bonded to the tooth 43.
Thanks to previous activations, the segment to be bonded to the tooth 41 has been lingually located and with the help of an utility probe has been displaced along the lingual surface of the tooth 41 and then bonded. The elastic return of the wire brought the tooth lingually as soon as the handles created space.
Also the segment of the wire to be bonded to the tooth 32 has been lingually located and positioned in the tooth through the employ of an utility probe and then bonded (Fig. 8).
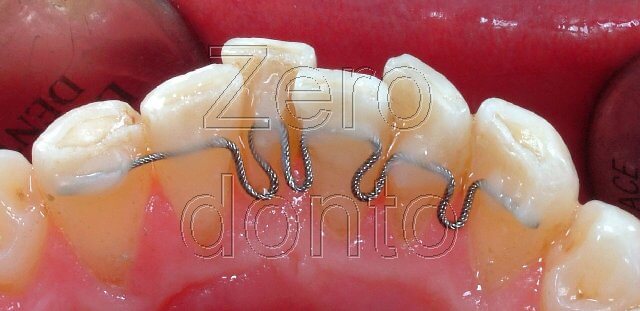
The alignment of the teeth in lingual-buccal direction has been achieved as soon as the handles expanded the canine arch.
Follow up
After one month we noticed a significant crowding reduction (fig. 9).
Checked the patient every 3-4 weeks, during every appointment the wire has been detached by the sector and activated consuming the composite with the employ of a cylindrical diamond bur mounted on a high-speed handpiece under water irrigation. The wire was activated opening the handles or bending it in lingual-buccal direction and then attached again.
When the levelling has been completed the active retainer can be replaced by a passive retainer, in this case after 6 months (fig. 10-14).

After one month since the passive retainer has been placed, evaluation of ortopantomography details showed no alterations related to the roots of the tooth elements involved ( fig.15).

References
1. Macchi A, Cirulli N. “Fixed Active Retainer for Minor Anterior Tooth Movement”. Journal of Clinical Orthodontics, 2000.
2.Macchi A, Rania S, Cirulli . “Una proposta per la gestione di disallineamenti anteriori: il mantenitore attivo di contenzione (MAC)”. Mondo Ortodontico, 1999.
3.Liou EJW, Chen LIJ, Huang CS. “Nickel-titanium mandibular bonded lingual 3-3 retainer: for permanent retention and solving relapse of mandibular anterior crowding”. Am J Orthod Dentofacial Orthop 119:443-9, 2001.
4.Musilli M. The Bracketless Fixed Orthodontics: nine years of clinical Experimentation. Prog in Orthod 9:72-91, 2008. 5. Mariniello A, Cozzolino F. Lingual active retainers to achieve teeth levelling in orthodontics: case series. International Dentistry SA Vol 10 N 5, pag. 24-29, 2008.
(FULL TEXT)
For further info:
zerodonto@gmail.com
